|
Today’s blog is about a critical role for the next Vice-President of AOTA; in fact it is a critical role for every occupational therapy practitioner and student.
BEING AN OCCUPATIONAL THERAPY ADVOCATE! For 33 years I have been an active advocate for occupational therapy, occupational therapy practitioners and our consumers. Each year, I participate in AOTA’s Capitol Hill Day. I have made 20 visits to Capitol Hill on Hill Day, in conjunction with AOTA Board of Director meetings and on personal visits to Washington D.C. This September I had the honor of acting as a mentor for two students who were making their first visit to the Hill. It was a wonderful experience. I am a longtime supporter of the American Occupational Therapy Political Action Committee (AOTPAC) and participate in the “two dollar a day” program. Last year I donated over $1,000 to AOTPAC. As Vice-President, I will continue to be highly engaged in advocacy. I will be highly engaged with AOTA members and non-members on social media, at State Association Conferences, at the AOTA Annual Conference & Exhibition and at other professional meetings such as the American Congress of Rehabilitation Medicine (ACRM) to encourage others to be active advocates. Please take a moment to visit www.aota.org/takeaction and spend a few minutes at the AOTA Legislative Action Center. Key issues currently being debated in Congress include the following (click the link to learn more):
Help me and other occupational therapy advocates to be more powerful professionals and take action now!
0 Comments
Recently a photo of a past AOTA Board of Directors (the Board) was reposted on social media. The picture was taken at the AOTA Vision 2025 Summit in 2015. The photo includes all elected members of the Board at that time and two appointed members. Because the photo was “shared” a second time, it was not immediately evident that the picture was of the Board or where, when, and why it was taken. The photo received several comments including two that asked (I'm paraphrasing) “Where is the diversity?” One of the comments pointed out that there was no one included in the photo who had an obvious disability. Looking at the photo (which I am in) it seems apparent that the members of the Board at that time all or mostly outwardly appeared Caucasian. There seemed to be a range of ages and four of the 14 persons in the photo appear to be male. I think it is accurate to say that there is no one in the photo who appears to have an obvious disability (although we know of course that many disabling conditions are not outwardly visible). I was a participant in both the Centennial Vision retreats and the 2025 Summit. For this reason these comments immediately drew my thought to where we stand with diversity as a profession. It is a complex issue that I cannot fully address in one Blog post. I am sure that I will leave out some important information to consider in the big picture, but I want to share my perspective as a Candidate for AOTA Vice-President. This is meant as continuing the conversation, not wrapping everything up with a neat bow. First a few comments about the concept of diversity in the Centennial Vision driven from my personal experience. From my experience I remember that while the idea of becoming a diverse workforce most certainly included increasing racial, ethnic and gender diversity the concept was much broader. The concept of diversity in the Centennial Vision was meant to include all types of diversity including issues such as broadening the types of work settings in which occupational therapy practitioners work and/or recognizing the diversity that second career professionals bring to the workforce. It included diversity in terms of disability status. There were also mentions of recognizing other forms of diversity that are not immediately outwardly identifiable and becoming a profession that is fully welcoming of types of diversity such as sexual orientation or gender identification. This explanation is not intended to lessen the importance or the challenge of increasing racial, ethnic and/or gender diversity, it is simply an explanation of the origin of the concept of diversity in the Centennial Vision based on my participation in the Centennial Vision retreats and on the Board. I also want to state that the participants at both the Centennial Vision retreats and the Vision 2025 Summit (both groups near 100) were in fact diverse in many ways. So how have we done in becoming a more diverse workforce? We have made some identifiable strides forward, but clearly not the type of changes we saw in other areas of the Centennial Vision such as “widely-recognized” or “evidence-based.” In terms of diversity of practice settings we maintain strong footing in established areas of practice such as hospitals, schools and long-term care and in fact the percent of the OT workforce in hospitals and LTC/SNFS increased from 37.5% in 2010 to 46% in 2015. This graph is taken from the 2015 AOTA Salary and Workforce Survey (Online at https://www.aota.org/~/media/Corporate/Files/Secure/Educations-Careers/Salary-Survey/2015-AOTA-Workforce-Salary-Survey-LOW-RES.pdf). 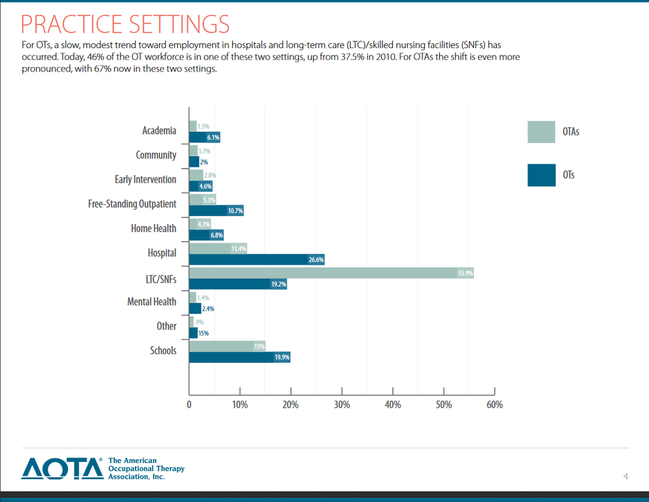 We have made forays into emerging areas such as primary care, population health and notably focused areas of practice such as oncology rehabilitation where I work. We certainly see many examples of creative practice with population such as refugees or the homeless. I continue to worry that we do not adequately support occupational therapy entrepreneurs and that private practice and business ownership receives less attention than it could. I am sure that many other examples of positives and areas for improvement could be mentioned. What about diversity in our students and new practitioners? I retrieved data through a search of AOTA Website on 12/6/17 and found a PowerPoint presentation with load date of 6/7/17 for a presentation given by Heather Stagliano (Director of Accreditation) and Neil Harvison (Chief Officer, Academic and Scientific Affairs) at the 2017 Annual Conference & Exposition in Philadelphia March 30-April 2, 2017. From 2000 to 2016 the number of occupational therapist students (including OTD) increased from 17,296 in 2000 to 20,627 in 2016 and the number of occupational therapy assistant students increased from 6,459 to 10,160 over the same time period. This next slide presents self-identified race according to the 2016 Annual Data Report from ACOTE. We can see that the percentage of students reported as white is approximately 75% overall. This is compared to 61.3% of people identified by the U.S. Census bureau in a population estimate for 2016 as “White alone, not Hispanic or Latino” (Retrieved Online 12/6/17 at: https://www.census.gov/quickfacts/fact/table/US/PST045216). 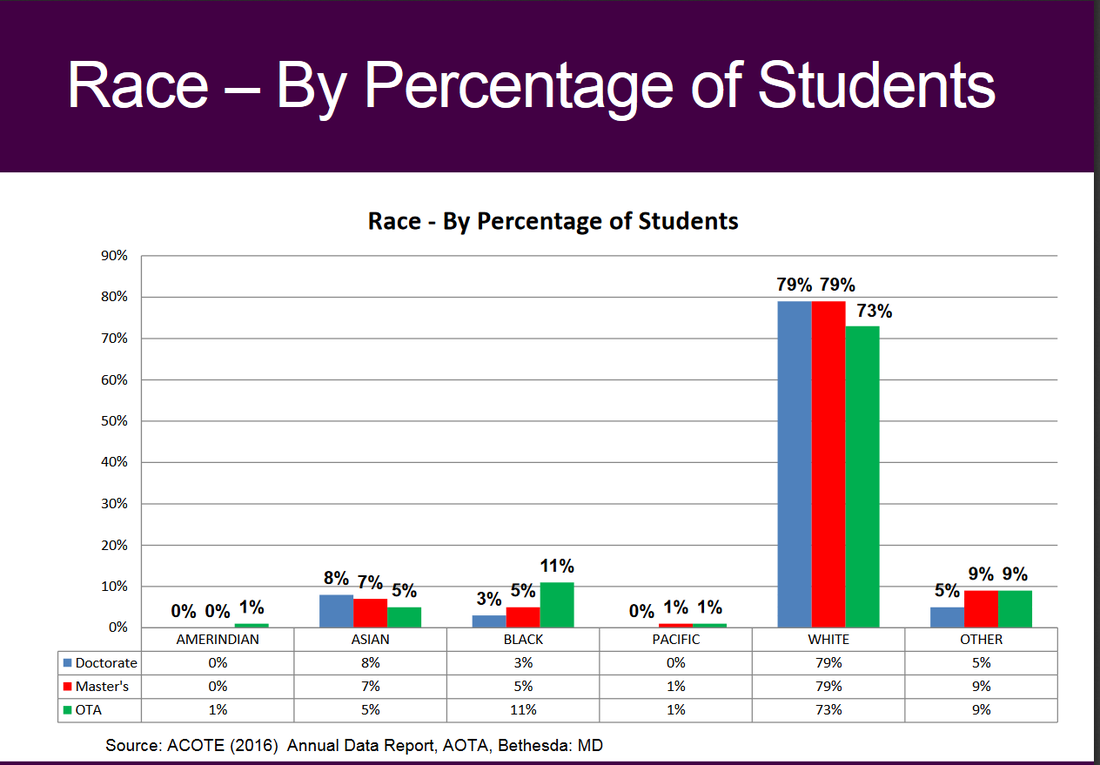 The next three slides show comparisons in percentages from 2010 to 2016 in those self-identifying as Hispanic, White, and Male. The next slide shows that the percentage of students self-identifying as Hispanic increased from 2010 to 2016. 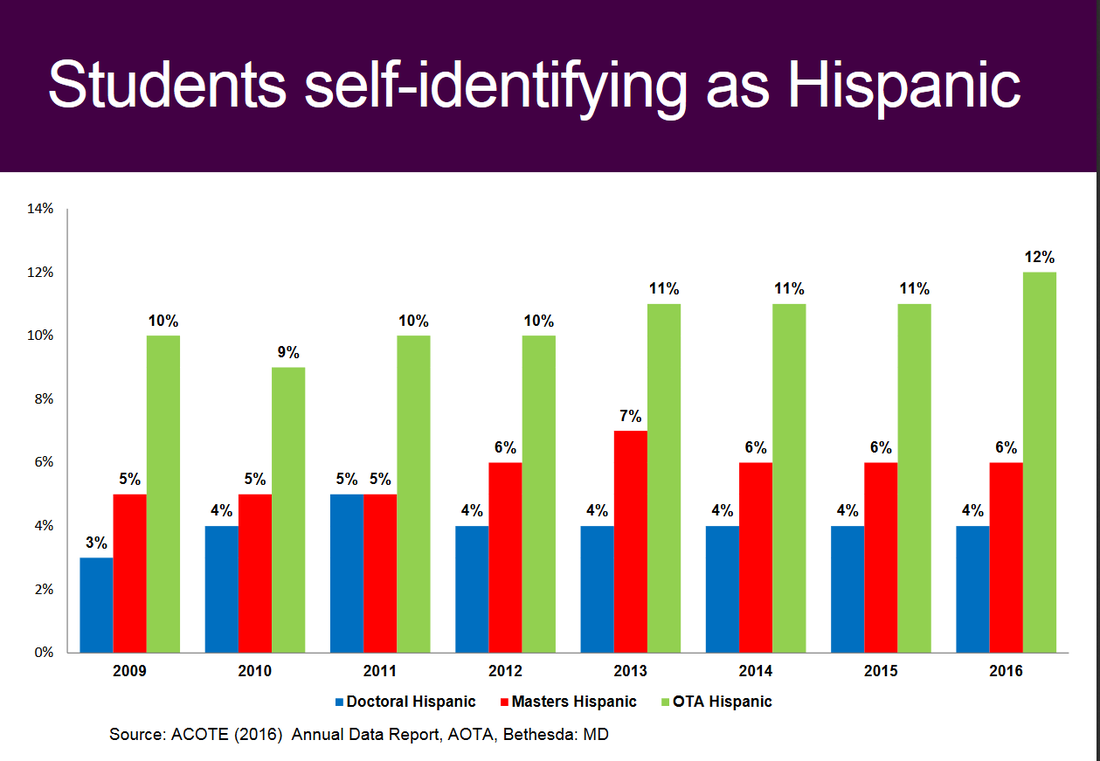 The next slide shows that the percentage of students self-identifying as White dropped from 2010 to 2016. . It is possible that some of this change could be explained by any changes in the categories included for self-identification (note that 5% of OTD students, 9% of Master’s students, and 9% of OTA students are identified as “other” in the slide on race from this report). 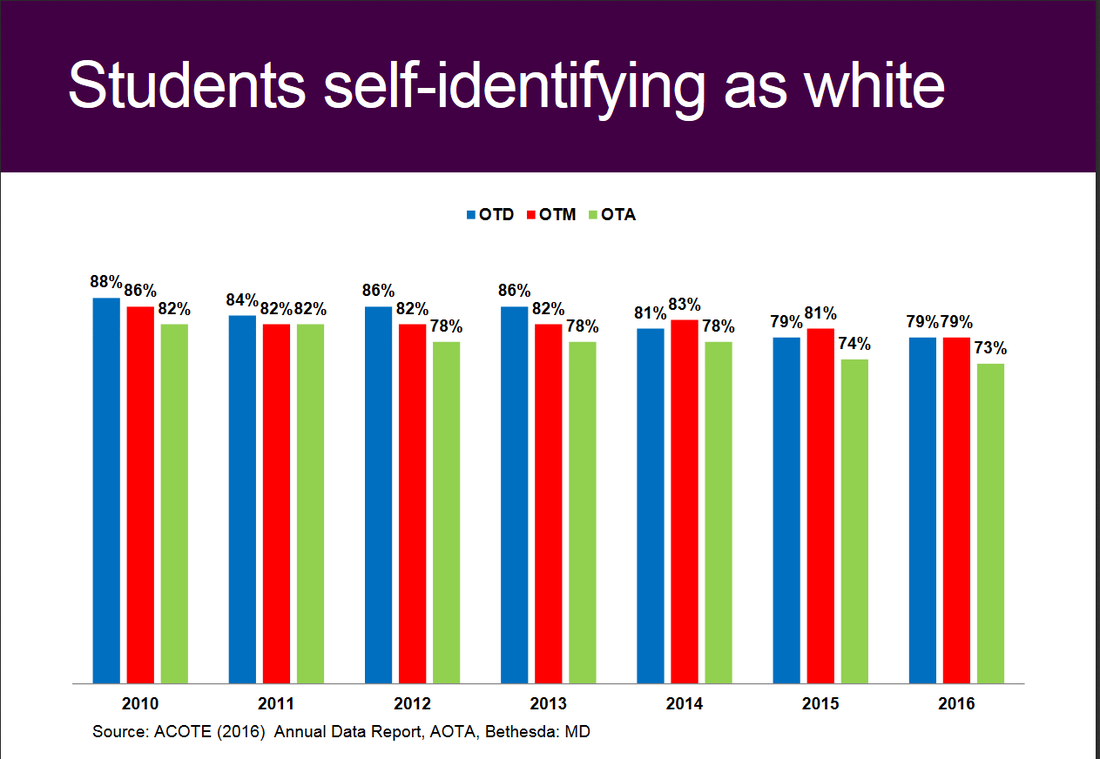 The next slide shows that the percentage of students self-identifying as male increased from 2010 to 2016 for OTD students, stayed the same for OTM students and dropped one percentage point for OTA students 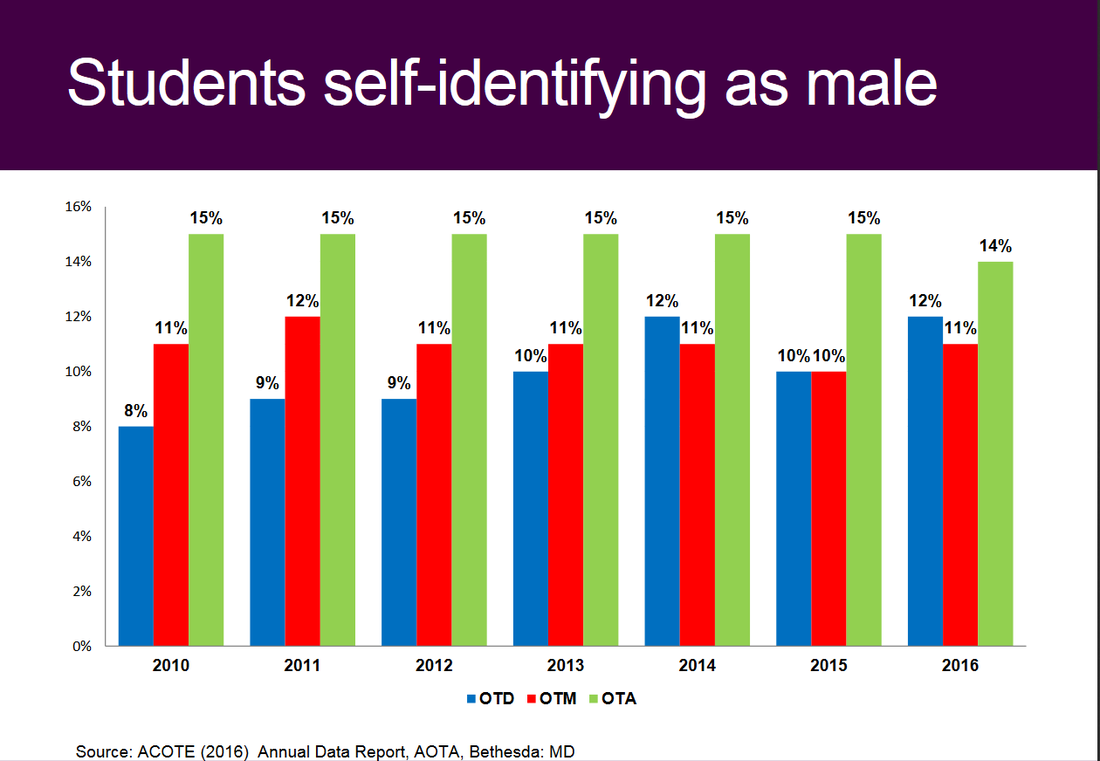 A full discussion of these statistics requires a deep dive far beyond the scope of this Blog post but I will summarize generally by saying that while we have made some improvements in these areas of diversity, I would characterize them as far from significant and leaving much room for improvement.
Before turning to some “so what” comments, I would like to comment on the issue of “obvious” or outwardly recognizable diversity and its complexity. Because I am included in the picture of the Board mentioned earlier and because I got to know my colleagues fairly well, I am positive that there are elements of diversity that are not outwardly apparent. These types of diversity are very important and should not be overlooked or undervalued. I want to avoid one of my pet peeves which is a “what about” response, meaning the tendency we have sometimes to respond to a concern about “A” with a response of “Yeah, but what about “B?” Still, diversity such as sexual orientation, gender identification, non-visible disability, ethnic diversity that may not be immediately outwardly recognizable ALL contribute in critical ways to making our workforce more diverse and more like the population in general. In this regard the answer to the question, “Where is diversity?” might be, “You’ll have to consider what you don’t see to see it.” So this Blog post has likely already run on too long, so let me get to the take-home, “so what?” messages that reflect some of my thinking as a candidate for AOTA Vice-President.
As a candidate for AOTA Vice-President I am committed to continuing attention and reinvestment of the efforts of the Board and the paid staff of AOTA in making our workforce more diverse. I would love to hear your ideas. Please contact me at bbraveman@gmail.com, friend me or message me on Facebook or let me know if you would like to set a time to have an Online chat or phone call. Thank you. Before you vote for any candidate in the upcoming AOTA elections you should know their answer to two simple questions:
Why do I want to be the next AOTA Vice-President? First I have a sincere passion and deep belief in the distinct value that occupational therapy can offer our society. Second I believe that the most effective way I can contribute to our profession is through volunteer service to my professional association. I became hooked on occupational therapy as a junior in high school. After watching the movie “Brian’s Song” about a football player with cancer I decided I wanted to be a PT and began volunteering at the local community hospital. I was assigned to acute care outpatient and almost all of the treatment I saw involved basic ambulation of patients and A LOT of crutch training for sprained ankles and broken legs. I became disenchanted and decided to stop volunteering but the astute PT asked me why and convinced me to try volunteering in OT. All it took was two observation visits and I was set on what I wanted to do with my life. I marveled at the creativity, problem solving and the focus on what I know understand to be client-centered care. I didn’t know it then, but the OTs always involved their clients in occupation-based intervention and we performed ADLs, cooked meals, problem-solved grocery shopping, planned for being safe at home and for getting around my hometown of Bangor, Maine. I was the sort of kid who always wanted to lead. I was Student Council Vice-President and President of the Bangor YMCA Leaders’ Club. I was a very young Supervisor at the Bangor City Pools and volunteered for leadership participation in almost every endeavor. As is consistent with my character, I completed one of my three Level II fieldworks at AOTA in the Division of Continuing Education and got my first exposure to AOTA volunteer leadership and staff close-up. I benefited from amazing mentorship over the first few years of my career by my fieldwork supervisor Susan Robertson who had high expectations and confidence for what I could achieve! My first AOTA conference was 1986 as a practitioner with one year of experience. I listened to Katherine (Kitty) Reed give her Eleanor Clarke Slagle Lecture on the “Tools of practice: heritage or baggage?” and heard AOTA President Eleanor (Ellie) Gilfoyle address the audience on “Professional Directions: Management in Action” and discuss the value of creative partnerships. My first conference was an extraordinarily impactful event. My early experiences convinced me that occupational therapy has amazing potential to address society’s needs and that I could contribute to achieving that potential. An example was speaking to a large audience at the Kennedy Center in Washington, D.C. who had viewed the groundbreaking made for television movie about teen suicide “Silence of the Heart” and explaining the contribution of occupational therapy to preventing teen suicide. These beliefs were also why I chose to volunteer to be the Vice-President and then President of the District of Columbia Occupational Therapy Association (DCOTA) after just four years of practice. The association needed someone to volunteer and I stepped forward. My entire career has focused on developing occupational therapy programs and promoting the profession to achieve our potential. Today my passion is Vision 2025 and guiding the profession through our next steps towards meeting society’s occupational needs. I envision supporting practitioners in established areas of practice such as school systems, SNFS and hospitals while also promoting emerging roles in practice settings such as primary care and population health initiatives. We can do both, there is no need to choose and I have experience in both camps. All of my experiences have convinced me that my greatest potential for contributing to achievement of an aspirational future for occupational therapy is as a volunteer leader. After 33 years of practice and experience as a State Association President, Chairperson of an AOTA Special Interest Section, Chair of the Special Interest Section Council, Speaker of the Representative Assembly (RA) and AOTA Secretary I am ready to take my next step in achieving my potential as a volunteer leader as AOTA Vice-President. Why should you vote for me? So I am passionate and committed…but is that enough? Why should you vote for me for Vice-President? The answer mirrors the story of my passion and commitment. Campaigns are not the time for modesty, so I hope you will appreciate my confidence and taking this opportunity to promote my skills and experience. I have served as a direct care clinician in inpatient rehabilitation, acute care, inpatient psychiatry, a neonatal intensive care unit, a skilled nursing facility and two work rehabilitation programs. I have a broad understanding of occupational therapy intervention in a wide variety of settings. Today I work leading nearly 100 OT and PT practitioners and am connected to the daily real life challenges of today’s health care environment. I have been a manager in a community-based hospital, a large academic medical center, an entry-level educational program (as Program Director) and now as the Director of the largest and first ranked cancer rehabilitation hospital and research center. I am an expert in management and the management processes of strategic and operational planning, financial planning and management, personnel development, mentoring and management, continuous quality improvement, outcomes measurement and marketing and promotion of occupational therapy services. This is a critical skill set for the AOTA Vice-President who has traditionally been responsible for strategic planning, evaluation of the AOTA Executive Director and oversight of the Centennial Vision (now Vision 2025) activities. I have been an educator in a masters’ entry program and several post-professional clinical doctoral programs. I developed and delivered multiple courses. I guided the fourth ranked occupational therapy program through the accreditation process and have deep familiarity and working knowledge of the accreditation standards, the accreditation process and of the culture and climate of higher education. I was a researcher and developed multiple occupational therapy interventions that were tested through the implementation of $1.2 million dollars of federal research funding. I served on multiple NIH grant review panels and have represented AOTA and occupational therapy on expert panels for NIH and the National Cancer Institute. I have skills in academic leadership having served as a Program Director in one of the top rated educational programs in the country. I have a demonstrated history as a practitioner scholar developing and implementing funded research combining qualitative and quantitative approaches to demonstrate the distinct value of occupational therapy. Through these experiences I gained an understanding of the challenges faced by our occupational therapy scholars and scientists and what AOTA and AOTF can do to support them. I have been a consultant to multiple community-based organizations and educational programs. I served for 6 years on the Board of Directors of the Alexian Brothers’ AIDS Ministry and have guided Boards of Directors, state OT associations and multiple faculty groups through strategic planning and visioning. I was involved in the development of both the Centennial Vision and AOTA Vision 2025 as an elected AOTA leader. I have been a staunch advocate for occupational therapy on Capitol Hill, at State Houses, in federal agencies and in communities. I have been a front line advocate and mentored others in the process of advocating for the profession. I have visited Congress on behalf of AOTA and the profession for 20 years and have mentored others in advocacy. I have been a steady volunteer for state associations and for AOTA and have continually asked, “How can I help? What can I do to contribute?” I have pursued a path of progressive leadership consciously making decisions about the next challenge that I can take on to make a difference and to gain a new set of skills as a volunteer leader. I will bring this skill set to my daily work on your behalf. I served in the Representative Assembly as SISC Chair, as Speaker and as Secretary for a total of 11 years. As Secretary I served on the AOTA Bylaws, Policies and Procedures Committee (BPPC) as we went through a major Bylaws revision. I know our official documents inside and out and few AOTA leaders can match my working knowledge of these documents. I have a solid understanding of the philosophical base of our profession, our core values and the processes of developing and implementing theory-driven, occupation-based and evidence-based occupational therapy interventions. I was recognized in 2017 with the AOTA Recognition of Achievement Award for my contributions in program development. It is wonderful that we have a vibrant slate of candidates for Vice-President. What sets me apart and why you should vote for me is the combination of the experiences that I have had and the multiple advanced skills sets I have developed over 33 years. This is the right time for me to commit to being a servant leader and to give all I can to AOTA and our profession. I hope that I have convinced you of this as well, and that you will vote for me to be the next AOTA Vice-President! Engaging and Promoting Occupational Therapy Assistants (OTAs) in AOTA Leadership and the Profession11/25/2017 For almost 15 years, I have listened to concerns, complaints and debates about how to increase the level of engagement and involvement of occupational therapy assistant (OTA) leaders in AOTA. The topic was debated in the Special Interest Sections in the early 2000’s when I served as Chairperson of the Special Interest Sections Steering Committee. It was debated in the late 2000’s when I served as Speaker of the Representative Assembly. It was debated more recently when I served on the Board of Directors as Secretary of AOTA and I am listening to concerns, complaints and debate today as I run for the office of AOTA Vice-President.
Over the last week, I have had four critical conversations with OTA educators and leaders and followed many more conversations on social media. I have reached out to occupational therapy assistant educational programs nationwide and I am beginning to hear from faculty. If we have not significantly impacted the perception and level of satisfaction with engagement and inclusion in AOTA of our OTA members and leaders over 15 years it is time for a new approach. I honestly believe that both the volunteer leaders and paid staff of our association value the contributions of OTAs and believe deeply in the potential for the future contributions to both established practice areas and emerging practice areas such as primary care and population health initiatives. I am fully convinced that both our volunteer leaders and association staff see OTAs as a critical piece of achieving Vision 2025. Still, it seems clear that absent a significant change, a new approach must be adopted. I would like to present an initial short list of actionable strategies that could be enacted to increase the engagement of OTAs in AOTA leadership. We need actionable strategies because as one OTA leader said to me (paraphrased), “I respect passion for occupational therapy, but I need to hear that leaders have ideas about what to do!”
This is just an initial list and I hope to hear more from OTA practitioners, educators. leaders and students about other actionable strategies we could take to engage occupational therapy assistants in AOTA leadership and the profession. Please send your ideas to bbraveman@gmail.com, friend me and/or send me a message on Facebook or contact me through www.brentbraveman.com. Also, please look for details on two “Listening Sessions” that I will be holding to give occupational therapy assistants the opportunity to share more ideas, concerns and feedback to me as a candidate for AOTA Vice-President. These sessions are schedule for:
If you would like to be sent an invitation to one of the listening sessions, please send my your Email address and the date that you would like to attend. Thank you to those of you who have shared your ideas! Brent What I bring as an occupational therapy researcher/scholar to and candidate for AOTA Vice-President.11/20/2017 In this post I would like present my experience as an occupational therapy researcher/scholar and describe how I can promote and support research and scholarship as the Vice-President of AOTA.
I have 33 years of experience as an occupational therapist and have knowledge, skills and experience that prepare me to advocate for the roles of researcher and scholar on the AOTA Board of Directors. I received my PhD in Public Health from the University of Illinois at Chicago in 2002. I received my first research funding as a doctoral student to develop and pilot a return to work program for people living with HIV/AIDS at the Howard Brown Health Center in Chicago. As part of the project I followed 16 men who completed the program for one year and used the data to complete my doctoral dissertation on a “Qualitative Study of the Subscales of the Occupational Performance History Interview.” In follow-up, my mentor and research partner Gary Kielhofner and I received funding for two federal research grants totaling $1.2 million dollars and carried out two more studies including the only two-group control study investigating the effectiveness of occupational therapy in return to work for this population to date. Our work influenced the delivery of work related services to persons living with HIV/AIDS nationwide and resulted in testimony before the National Institute of Medicine Committee on Social Security HIV Disability Criteria in 2010. In addition to my own research, I sat on NIH review panels 9 times including the Small Business Technology Transfer Program and a panel on Stigma and Global Health. I have participated as an invited subject matter expert on the “National Cancer Institute Evidence-Based Approaches for Optimizing Employment Outcomes among Cancer Survivors” in 2016 and the “National Institutes of Health Subject Matter Expert Panel on Cancer Rehabilitation" in 2015. In March of 2018 I will serve as an invited participant to the American Occupational Therapy Foundation (AOTF) Grant Planning Workshop focused on aiding cancer survivors to engage in work and daily life roles.” During my 19 years at UIC I served as the Program Director for the entry-level educational program and collaborated with our tenure-track faculty closely. I gained much experience and familiarity with the challenges of pursuing all levels of funding while balancing research with teaching and other academic duties. As a scholar who has authored two text books, 22 peer reviewed journal articles and 15 book chapters I have an appreciation for the hard work and contributions of the researcher/scholars in our profession. As Vice-President of AOTA, I will bring my knowledge and experience of the research process, along with my passion for occupational therapy and represent researchers on the Board of Directors, to the American Occupational Therapy Foundation, and to funding agencies that support the development of evidence for the value of occupational therapy interventions. I will be a strong voice for the need to promote the development of new researchers, post-doctoral experiences and mentoring of students to pursue a career in science in the field of occupational therapy. I will work to develop new opportunities to support academic-practice collaborations to promote a scholarship of practice. I hope that you will consider casting your vote for me. Do not hesitate to contact me if you have questions, concerns or feedback you would like to provide through this website or at bbraveman@gmail.com Brent Progressive Leadership: My Leadership Journey
As attention to the upcoming AOTA elections has increased I have read multiple comments about the length of service for some of us who have a passion for volunteering for our state and national professional associations. Not all of the comments were complimentary. Some were about the same folk just swapping seats, and one described the process as inbreeding (Yikes!). This prompted me to want to share the story of my leadership journey. I see my leadership journey as one of progressive leadership; an intentional effort to assume increasingly more important roles as my professional knowledge, skills and potential to contribute has increased. I was extraordinarily lucky to have excellent mentorship early in my career. Even as a student I knew I wanted to be involved in the profession on a national basis. I chose to do a Level II fieldwork at AOTA and completed it in the Department of Continuing Education. My supervisor Susan Robertson became my first mentor. She encouraged and challenged me to get involved! With just four years of experience, I ran and was elected first for Vice-President and then President of the District of Columbia Occupational Therapy Association. I have to be honest, the DCOTA was reconstituting itself at the time after having been disbanded, and both times I was on the ballot I ran unopposed! Still, as a practitioner with limited experience I think it tells you something about my enthusiasm and drive that I put myself forward and assumed the leadership of a State Association. As perhaps the youngest member of what was then called the “Committee of State Association Presidents (CSAP)” I learned a tremendous amount. I started to gain an understanding of the importance of state associations and the relationships between state associations and AOTA. I was introduced to the structure of AOTA and the influence that leaders can have on the profession through advocacy and clearly and logically articulating a point of view. It fired my interest in volunteerism and I was hooked on volunteering for AOTA. I recently found a quote about failure that rings true for me. The quote is that “failure is delay, not defeat (Lax, 2016).” Not every step on my journey has been smooth. In fact my next step on my journey was running for the Chairperson of the Administration and Management Special Interest Section (AMSIS). I lost that election, but was asked to serve on AMSIS as the Education/Research Liaison and I jumped at the chance. My education about the association and about the needs of AOTA members continued and three years later I ran for AMSIS Chair again, and won. As AMSIS Chair I had the opportunity to serve on the Special Interest Sections Steering Committee (SISSC) that coordinated much of the activities of the SISs. This gave me the opportunity to learn about occupational therapy practice in a whole new light. I began to understand the cross connections between various practice areas, the challenges we shared and what each group uniquely contributed to the distinct value of occupational therapy. I also gained exposure to a group of leaders who each had their own style and set of skills and in turn this helped me develop. In 2003, the Chair of the SISSC resigned because she accepted a paid position for AOTA. AOTA President Mary Evert asked me to assume the position and I served as the appointed SISSC Chair for two years and then chose to run for the position and was elected to a three-year term in 2005 as Chair of the renamed Special Interest Sections Council (SISC). The five years in this position were amazing and contributed more than I can describe to my development as a leader. For five years I sat in a voting position in the Representative Assembly (RA). I learned about AOTA policy and procedure, how association policy is developed (the good, the bad and the very confusing!), and gained a deep understanding of how our very small but incredibly skilled AOTA staff support the volunteer leadership. I made mistakes as a leader and grew from them and gained insight into my strengths and weaknesses as a leader. For the first time I had the opportunity to dip my toe into mentoring and providing support to less experienced volunteer leaders who were coming up behind me. My next step in progressive leadership was to run and to be elected to be Speaker of the Representative Assembly (RA). This was a significant accomplishment and challenge as an occupational therapy leader. I did not “grow up” in the RA and had not served as a representative (RA Rep). Because I have served as a voting member of the RA for five years I did not consider it an obstacle that I had not served as a Rep and was surprised by the resistance I encountered by some to my candidacy. Shortly after being elected, a long-time volunteer in the RA challenged me by asking me, “Why are you here? Why did you run for Speaker and what do you want?” I realized that with each progressive step in Association leadership, I need to prove myself both in terms of skill and in terms of commitment and motivation. Serving as Speaker of the RA was perhaps the single most valuable learning experience I’ve had in volunteer leadership. Guiding 80ish voting volunteer members through a structured decision making process (Robert’s Rules of Order and parliamentary procedure), coordinating the contributions of multiple bodies of the association and negotiating participation by volunteer leadership and paid staff and serving on the Board of Directors……whew! One of my contributions to the RA was to make some changes in operations for the better such as streamlining the way we processed minor changes to documents or documents that were reviewed and did not require any change. Like all AOTA bodies, I had a staff liaison that had staffed the RA for some time. On several occasions I would ask, “Why do we do it that way?” I would listen to the answer which sometimes included “It's the way its been done” and would reply, “Okay, we are not doing that, this is what we are going to do….” I learned A LOT about facilitating change in a complex organization. I also learned a lot about being a leader who cannot always say everything you would like to say. On multiple occasions I was asked what I thought about a controversial issue coming before the RA and my answer had to be, “As Speaker I do not have an opinion, my job is to assure fair debate and transparent decision making.” Boy that was hard! I learned that often members want leaders to listen, not speak. I continued to learn more about how AOTA is organized and about the complex process of coordinating decision-making by volunteer leaders and the work product of AOTA paid staff. Perhaps most importantly I had a crash course in responding to the breadth and diversity of AOTA member feedback. During face-to-face RA meetings at annual conference it was not uncommon to be crossing a hotel lobby and to encounter a member who would give you their passionate opinion about what should happen with a motion before the RA, only to walk 50 feet and encounter a member who gave an equally passionate opinion about why the opposite action should be taken on the same issue! One major challenge that I faced and handled successfully during my term as Speaker, was making the decision to cancel a face-to-face meeting at the 2009 Annual Conference and hold the meeting entirely Online. This decision was made in conjunction with AOTA President Penny Moyers and AOTA Executive Director Fred Somers as a response to the dire budget situation following the market crash of 2008. AOTA took a big hit to its investments and had to find ways to eliminate expenses until they recovered. Penny and Fred scheduled a phone call with me and when I found out that we could save $150,000 by holding the face-to-face meeting Online, I quickly said, “I’ll find a way to make it work” and we did. It took many hours of work and several weeks of late evenings and early mornings but the RA Leadership Team and our AOTA staff Liaison pulled it off. I learned a lot about the need and the capacity for volunteers to be flexible when something really important is on the line! My next attempt progressive leadership was to run for the office of Vice-President. The Vice-President plays a major role in guiding strategic planning for the BOD, chaired the Centennial Vision Commission and led the annual performance evaluation of the AOTA Executive Director. These are activities that I am well suited for based on prior experience. I have led multiple groups including non-profit organizations, a faculty and state associations in visioning and strategic planning activities. My first run for VP did not work out and I lost the election to Amy Lamb who did an amazing job as VP and is now our President. While I was disappointed at not becoming VP, I decided to jump right back in and was elected as AOTA Secretary the next year. As Secretary I served on the Bylaws, Policies and Procedure Committee (the BPPC). While this might not sound like a lot of fun, it is an invaluable experience. As Secretary I became intimately familiar with the Bylaws and the policies and procedures that guide all AOTA activities. This is a knowledge and skill set that is very helpful for AOTA leaders who are often faced with complex situations and have to devise action plans that are not only ethical and effective, but that also follow the rules set out the Bylaws, policies and procedures. During my term the BPPC completed a major overhaul of the Bylaws, policies, procedures due to a change in the law that governs AOTA incorporation in the District of Columbia. After serving as Speaker of the RA and as Secretary, there are few volunteer leaders who have the depth of understanding that I have of the documents that guide the operation of our Association. So here I am in 2017, and making another run for the Vice-Presidency and taking the next step on my progressive leadership journey. I am doing so because I am passionate about occupational therapy and about our professional association. I believe that the biggest contribution I can make to occupational therapy is through volunteer leadership. Each step that I have taken in my journey has added to my knowledge, skills and capacities to serve as Vice-President. I hope my journey illustrates that progressive leadership is a lot more than just swapping seats and that my journey has prepared me to take this next step and to be successful. I would be honored to serve as your Vice-President and you have my pledge that I will be fully committed, accessible and engaged with you, the members. I have adopted this personal mission statement: I will be a servant leader and AOTA Vice-President who is constantly engaged and accessible to AOTA members working tirelessly to meet member needs and to achieve AOTA's Vision 2025. Please reach out to me with any questions, concerns or suggestions. You can Email me at bbraveman@gmail.com, friend me on Facebook, send me a tweet at @brentbraveman or check out my personal webpage to learn more about me at www.brentbraveman.com. I have been listening to occupational therapy practitioners and reading a lot about concerns over the ACOTE mandates to move to a single point of entry for the occupational therapist at the doctoral level and for the occupational therapy assistant at the baccalaureate level by 2027. One issue that I am gravely concerned about is one gap in thinking between some of those who support these moves and some who oppose it. This gap has to do with thinking about what these changes mean, why they are being proposed and about how we value the skills, knowledge and experience of seasoned practitioners.
Many of those who support the mandates focus on the possibilities for changing the knowledge and skills of the entry-level practitioners we graduate. The thinking is that we can reform our educational programs to prepare graduates to move into leadership roles in existing practice settings more quickly and to be better prepared for practice in evolving settings. Essential to this line of thinking is that we not just “tack on” an additional semester or two, but that we reformulate the accreditation standards to provide content that supports entry-level practitioners thriving in the practice settings and environments of 2027 and beyond. One theme I am hearing among the concerns of some who oppose the mandates is that they are perceiving the message that the knowledge, skills and critical reasoning abilities that they have gained over years of practice is not being valued; that advanced degrees are being valued more than experience. It strikes me that regardless of how we move forward as a profession and regardless of whether you support or oppose the mandates, this is a perception gap that we must close. My occupational therapy degree is at the baccalaureate level in 1984. I went on and obtained a Master’s degree in 1992 and a research doctorate degree in 2002. I chose to obtain advanced degrees because I perceived that they would provide me skill sets I did not obtain in my entry-level education and open doors to roles and opportunities that would not be accessible to me with my entry-level degree. I do not remember if there was expressions of concern over not valuing experience equally with a graduate degree as the profession debated the move to a post-baccalaureate level. They may have existed and I was just not tuned in to them at the time. However, I am sure that I never had concerns that my years of experience (which would have been 13 in 2007) would not be valued. I have worked in one form of administrative role or another since 1989 and have frequently been in the position of evaluating candidates for hire or other opportunities. While I value what advanced degrees bring to a candidate, they do not replace experience. I have perceived that many entry-level candidates with an OTD (or DPT, as I am responsible for a large rehabilitation department) have skills that students prepared at the masters level do not (it depends on the programs!). Still, I have never perceived the clinical doctoral degree as any form of substitution for the skills, knowledge, critical and professional reasoning that comes with years of practice. If we are open to, or especially interested in an entry-level practitioner than the OTD may be a tipping point on the scale, but if we need experience, the clinical doctorate has never been seen as equal or a substitution. Many times now I have read the questions, “What is wrong with our students now?” or “What is the problem with the quality of our current education?” More often I am hearing the question, “What is lacking that my years of experience won’t satisfy?” My answer has been that if we move forward with the OTD as the single point of entry for the occupational therapist, it has to be about preparing for a different future. It is NOT a reaction to a problem now or to fix any issue with quality, but about graduating a different type of entry-level practitioner for a future that will require a different set of entry-level skills. I appreciate that many members of the profession think that the move is unnecessary or that it will not achieve the desired outcome for one reason or another. Debate on those issues as well as other pros and cons is important and should continue, and as much as possible should be driven by data, the highest quality evidence available, and sound logic. However, I think that as the debate continues it is critical that our messaging and our common understanding changes. We need to acknowledge clearly and loudly that, experience matters. If you are a baccalaureate or masters educated practitioner with years of experience under your belt, you offer the profession something than cannot be replaced with any advanced degree. Your skills, knowledge and capacity for reasoning are golden, and you should hear loud and clear that you critical to our future, and part of the solution. You are not a problem to solve and we cannot replace you. If that message has not been clearly conveyed, as someone who has advocated for moving to the OTD as entry-level, I apologize and seek to correct the record. I would love to hear others’ thoughts questions and concerns. Please feel free to email me at bbraveman@gmail.com, friend me on Facebook, send me a tweet at @brentbraveman or contact me through my personal website www.brentbraveman.com. I have been asked about my position on the mandates by the Accreditation Council on Occupational Therapy Education (ACOTE) to move to a single point of entry for the occupational therapist at the doctoral level and for the occupational therapy assistant at the baccalaureate level by 2027. I think it is important for candidates for AOTA leadership positions to be engaged and respond to requests from members to share their opinions, positions and thinking. These are complicated issues so a thoughtful response cannot be given in 140 or 280 characters!
I have been having conversations with occupational therapy practitioners and students at several conferences and events and reading communications on social media. I have seen and heard numerous references to the importance of transparency; so let me begin there by being transparent about my past activities related to a single entry-level for the occupational therapist. I served on the AOTA Board of Directors (BOD) from 2013-2016 including the time when the BOD issued its position statement on moving to a single point of entry for the occupational therapist at the doctoral level. In fact, I led one of the Ad Hoc committees that led to the BOD assuming its position and agreed to coordinate communication on behalf of the BOD on OTConnections. It was not an easy decision. There were clear pros and cons and I have stated on numerous occasions that thoughtful and informed members interpreted the same information differently and reached a different conclusion. At that time, and today, I believe that what would serve the profession the best in the long term would be moving to a single point of entry at the doctoral level for the occupational therapist. My personal rationale was largely in line with the rationale provided by the BOD in 2014 and you can find information at https://www.aota.org/AboutAOTA/Get-Involved/BOD/OTD-FAQs.aspx. While I favor ultimately moving to the OTD entry-level for the occupational therapist, I also think that how we get there is critically important. I believe that while the position of the BOD or any other decision making body is important, the process for making a decision on critical issues such as these is more important. In 2014 the BOD issued its statement AND called for a profession wide dialogue. It then set about creating numerous opportunities and venues to facilitate that dialogue. Despite attempts to convince members of the profession, consensus was not achieved and ACOTE made a determination to keep entry at two points. The process the BOD used was transparent and while not everyone had the same interpretation of data and information, it was clear how the BOD came to its position and what the position was based upon. We engaged with membership, answered questions and listened to those who shared the same position and those who did not. I was surprised by the announcement that ACOTE had voted to mandate changes in the entry-level requirement for both the OT and the OTA. To my knowledge, ACOTE used its independent decision making authority and no one including the current BOD received notice in advance of ACOTE’s announcement. I do not currently have enough information to voice my support for changing the entry-level requirement for the OTA to the baccalaureate level and I have more concerns about the down sides than I did with the decision for the OT. Like the move to the OTD, I can see clear advantages and disadvantages, but I do not have access to a clear rationale used by ACOTE and have many unanswered questions that I expect should be answered by a clear report by ACOTE. I am pleased that ACOTE has responded to concerns of members and non-members, has held the move in abeyance and is collecting feedback. Despite my belief that the best interest of the profession would be to ultimately move to the OTD entry for the occupational therapist, I would support a similar decision by ACOTE in this regard at this time. The expectation of being provided a clear report on the data, information and other forms of evidence used to make determinations is appropriate and should be forthcoming in regards to both mandates. In the absence of these reports, I cannot voice my support for moving forward with the mandates. Finally, I want to express my thanks and respect for the members of the BOD and of ACOTE for their service. Whether I agree or disagree with any individual decision by either body, my experience with members of both groups over the years has been extremely positive. Calls for more information and transparency in regards to the decision making process are reasonable. However, I am disappointed and disheartened to read and hear some suggestions that members of these bodies are acting with anything but the best interest of the profession in mind. Moreover, in my two terms serving on the BOD as Chairperson of the SISSC Council and as Secretary, I saw nothing to indicate that the independent decision making authority of ACOTE was not in place in full force. I hope that I have stated this clearly, but understand that there may additional questions. I am happy to answer questions, but am not involved in advocating any other action that those I have stated here at this time. It’s been a while since I have written a blog post. Work and life in general have been keeping me pretty busy, and frankly world and national affairs have made me want to stick my head in the sand. I've felt a little blah. However, this is something I care about deeply, so I’m baaaaaaaack! Dear AOTA Members, You currently have the opportunity to give feedback on the draft of an official paper on “Occupational Therapy’s Role in Population Health.” Population health is central to AOTA’s Vision 2025 statement. The vision statement is: “Occupational therapy maximizes health, well-being, and quality of life for all people, populations, and communities through effective solutions that facilitate participation in everyday living.” Giving input and feedback on official documents is one simple way that every member of AOTA can play an active role in guiding the future of our association and our profession. I have a strong investment in occupational therapy practitioners addressing population health as one part of our varied practice. I took the time to organize and present my ideas in an article available in open access in the American Journal of Occupational Therapy titled, “Population Health and Occupational Therapy. You can access the article here: https://ajot.aota.org/article.aspx?articleid=2478827&resultClick=3  I was honored to be invited to participate as a presenter at an institute on population health at the 2017 Annual Conference & Exhibition and was instrumental in starting a discussion on population health on OTConnections. AOTA members can read that discussion here: https://otconnections.aota.org/sis_forums/f/7926.aspx I was fortunate to be serving on the Board of Directors of AOTA during the development of the Vision 2025 statement and am extremely proud of the extensive process we used to develop the statement and get feedback. Here is a brief description of the process located on the AOTA Website. “In 2014, AOTA began the new visioning process by retaining McKinley and Associates to solicit and organize input from within the profession and from outside stakeholders. This included broad-based surveys to more than 60,000 member and nonmembers, and interviews with industry leadership, all seeking insight on the profession’s challenges, strengths, and potential goals. McKinley reported their findings at the AOTA Vision Summit, held in October 2015. The Summit brought together just fewer than 100 AOTA staff and volunteer participants, invited to represent a broad range of age, experience, diversity, and practice settings. Over 2 days, the group reviewed McKinley’s research, and also discussed pertinent societal trends and potential changes shifts in health care. The Summit concluded with defined “essential elements” and three drafts of a possible new vision statement. Those drafts were vetted and distilled into a single statement, which was sent to 58,000 practitioners and students, who responded with a 78% approval rating. The Board adopted and approved Vision 2025 at their February meeting” (AOTA, 2016). It is understandable and predictable that not every occupational therapy practitioner and not every member of AOTA supports this statement. But the fact that 78% of those who responded to the survey rated the vision statement as favorable or highly favorable is significant. If you are not yet familiar with population health as area of intervention for occupational therapy practitioners it is important that you take the time to learn about it and form an independent position. I’ve shared my thinking (in my AJOT article) and encourage you to listen to the viewpoints of others, including those who disagree with me. It is important also that you question the validity of information that is presented. For example I recently saw this slide posted on social media. It reflects the results of one question from the survey sent to 58,000 practitioners and students. The question was “Please rank each of the phrases below according to their importance on the overall impact of the vision statement.” 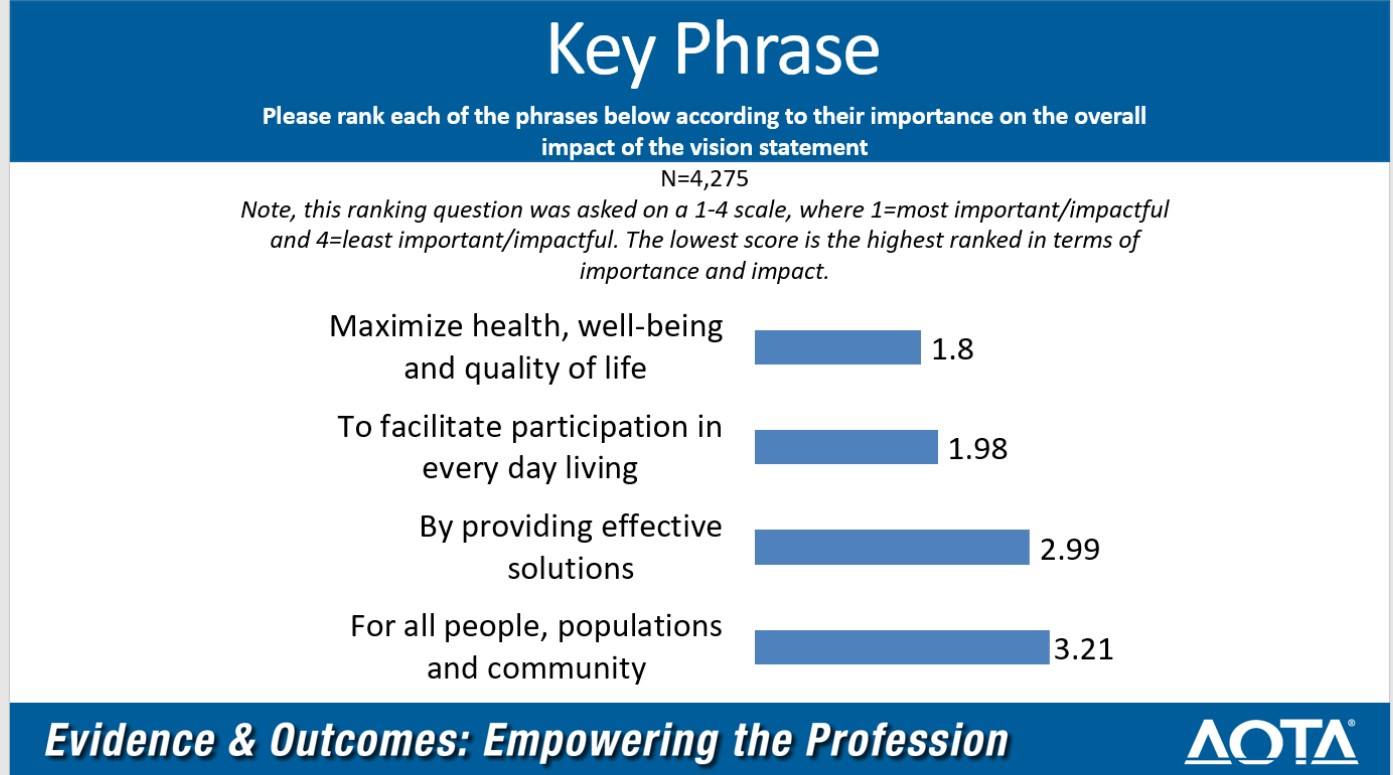 The inference presented on social media seemed to be that the results of this question indicate that the respondents did not think that the phrase “for all people, populations and community” was important. But of course we don’t know that. What we know is that when presented a forced ranking option the key phrase “for all people, populations and community” was less important than three other key phrases in the Vision 2025 Statement. If the same respondents were asked to rank each of the four key phrases along a continuum of very important to not at all important, it is possible that many of them would rank all four key phrases as important to the overall impact of the vision statement. Given that 78% of survey respondents rated the vision statement as favorable or highly favorable I don’t believe they had a negative reaction to any of the key phrases.
I was in the room at the Board of Directors meeting when the representatives of McKinely Associates reviewed the process for developing the statement and for review of stakeholder feedback including the survey and focus groups with almost every leadership body in the Association. The results and positive response to Vision 2025 were compelling. Any suggestion that AOTA has moved forward without listening to its members has no grounding in reality or fact. Again, if you are an AOTA member I highly encourage you to visit the AOTA website and read about Vision 2025 and population health. I encourage you to read the draft statement on the role of occupational therapy and population health and provide feedback. Thank you! American Occupational Therapy Association. (2016). AOTA Unveils Vision 2025. Online at: https://www.aota.org/AboutAOTA/vision-2025.aspx Like the vast majority of the approximate 14,000 attendees, I had a wonderful experience at AOTA’s 2017 Annual Conference & Exposition in Philadelphia celebrating the 100th anniversary of occupational therapy. It was joyful to catch up with colleagues, network, make new professional connections, learn and share my experience in three presentations I was involved in delivering. One of those presentations was a Pre-Conference Institute titled, “Supporting Occupational needs Through Population and Organizational OT: Gain Knowledge and Skill to Expand Your Practice.” This institute was organized by Roger Ideishi, JD, OT/L, FAOTA who is an Associate Professor of Instruction in Rehabilitation Sciences & Program Director at Temple University. Roger led 13 faculty including myself in delivering this six hour learning experience with an enthusiastic audience of occupational therapy practitioners who are either interested in, or currently providing population-based occupational therapy interventions.
Population health is a key component of the American Occupational Therapy Association’s (AOTA) Vision 2025 which reads: “Occupational therapy maximizes health, well-being, and quality of life for all people, populations and communities through effective solutions that facilitate participation in everyday living (AOTA, 2106).” The genesis of Vision 2025 can be found here: https://www.aota.org/AboutAOTA/vision-2025.aspx. It is important to note that the new vision statement was developed over an extended period of time through a process that offered tens of thousands of occupational therapy practitioners and other stakeholders the opportunity to provide input and feedback. The draft of the statement was sent to 58,000 practitioners and students and met with a 78% overall approval rating. This of course means that there is not universal approval and that some members of AOTA and non-members of the association object to part or the whole of the statement. Nonetheless, population based intervention has been endorsed as an appropriate area of intervention for occupational therapy practitioners by the official bodies of the association including the Representative Assembly. For example, AOTA’s (2013) official statement on Occupational Therapy in the Promotion of Health and Well-Being includes a section on a population health approach and states, “In addition to providing occupational therapy interventions for individuals, occupational therapy practitioners can develop and implement occupation-based population health approaches to enhance occupational performance and participation, quality of life, and occupational justice” (AOTA, 2013, p. S49). The 3rd Edition of the Occupational Therapy Practice Framework: Domain and Practice clearly establishes communities and clients as populations and establishes the appropriateness of population-based interventions to address the occupational needs of populations (AOTA, 2014). At the end of our Institute the faculty and the attendees discussed strategies for keeping participants in touch with each other and for finding a structural home in AOTA. I volunteered to explore options and one simple step that has already been accomplished was to create a permanent discussion thread in the AOTA Member Forums area on “Population Health.” If you are a member of AOTA you can find the discussion here: https://otconnections.aota.org/sis_forums/f/7926.aspx. If you are an AOTA member and are not yet a participant on OTConnections all you have to do is create a free account. We are interested in having a thought provoking and respectful interchange about the development of effective population-based occupational therapy interventions around the globe. While there are already occupational therapy practitioners providing creative, innovative and effective population-based interventions in a variety of areas we have much to do to move our way forward in this area of intervention. Some of these needs include:
I’m already on the road to 2025. I hope you join me and others and help to shape the journey! References: American Occupational Therapy Association. (2014).Occupational therapy practice framework: Domain and process (3rd ed.).American Journal of Occupational Therapy, 68(Suppl.1), S1–S48, http://dx.doi.org/10.5014/ajot.2014.682006. American Occupational Therapy Association. (2013). Occupational therapy in the promotion of health and well-being. American Journal of Occupational Therapy, 67(6, Suppl.), S47–S59, http://dx.doi.org/10. 5014/ajot.2013.67S47. |
The opinions expressed in my blog are personal and neither represent the views of my employer nor any organization.
Archives
July 2023
Categories |

 RSS Feed
RSS Feed
Proudly powered by Weebly