|
I genuinely appreciate the opportunity over the last 10 days that I have had to engage in dialogue with others and to reflect on the topic of diversity in the occupational therapy profession; especially diversity in representation in leadership in our professional association. On December 6th I published a blog post titled “Where is the diversity?” (https://www.brentbraveman.com/blog/where-is-the-diversity) and posted a link to it on Facebook. The blog post has the highest readership of any blog post so far on my website. There have been over 800 unique readers and the Facebook post resulted in quite a bit of discussion. Since then, a number of AOTA members including several students and young leaders in AOTA have also sent me Emails and personal messages to express concerns and share their experiences, opinions and perspectives. One of the students who Emailed me described some of the comments on Facebook as initially “heated” but gave me props for responding calmly and creating opportunities for dialogue and learning. I hope that is true. I hope that I asked relevant questions to help me understand, and I hope that I listened and learned. Several of the folks who have contacted me have referred me to resources and blogs by others who have shared perspectives on diversity in the profession and in our leadership. Reading first person narratives has been incredibly instructive and impactful. I am going to reach out to some of these folks and ask if they are okay with me calling attention to their blogs and sites. I hope that others will use their voices and that the dialogue continues and grows. I have added a page on “Diversity in Occupational Therapy Blogs and Resources” on my website https://www.brentbraveman.com/diversity-in-occupational-therapy-blogs--resources.html. If there is a blog or resource you think I should add please send me the link. What did I hear and learn over the last 10 days?
I am pretty sure I already knew that last one, but it is good to get a refresher every once in a while and to be reminded of the importance of asking questions and listening. I was also reminded that while I can pull from my own experiences as a member of the LGBT community to empathize with the experience of others, it only takes me so far. Like all of us, I have many traits and characteristics and whatever discrimination I have experienced as a member of the LGBT community has been tempered by also being a white man in today’s society. The experiences of women, of persons of color and of persons with disabilities within the profession have some similarities to my experiences but there are more differences that I can only hope to appreciate if I work hard at listening and understanding. It is tempting to offer a bulleted list of solutions and a path forward. I have some ideas, and shared some of them in just such a bulleted list in my initial blog post https://www.brentbraveman.com/blog/where-is-the-diversity (and other suggestions have been provided by some of the members who have joined the dialogue in the last 10 days). After all, I am trying to convince members to cast their votes for me to be the next AOTA Vice-President, and, I tend to be action oriented; but after reflecting on the dialogues that I have been involved in over the last 10 days I think that making two commitments is the most important thing I can do.
Thank you to those of you who have spoken out in the last 10 days and I invite others to join in. Thanks! 
0 Comments
Advocacy Week: Call Congress Today to Ask Them to Act on the Therapy Caps Before January 1st!12/16/2017 As the next Vice-President of AOTA I will be a tireless advocate for occupational therapy practitioners and consumers of occupational therapy! All this week is advocacy week at www.brentbraveman.com and each day I am highlighting a critical piece of legislation address at the AOTA Legislative Action Center. Today I am going to revisit a critical issue a second time because we are very close but Congress must take action before January 1st to end the therapy caps! Please call your Senators and Representatives today and tell them you want them to act now so that the arbitrary therapy caps do not go into place on January 1! Visit this link and enter your Zip Code to get the numbers of your Senators and Congressional Representative. The screen shot below shows you that all you need to do is enter your Zip Code! http://capwiz.com/aota/callalert/index.tt?alertid=79352641 Join me, AOTA and AOTPAC and your colleagues and Take Action Today!  As the next Vice-President of AOTA I will be a tireless advocate for occupational therapy practitioners and consumers of occupational therapy! All this week is advocacy week at www.brentbraveman.com and each day I am highlighting a critical piece of legislation address at the AOTA Legislative Action Center. The Lymphedema Treatment Act is a piece of legislation that is near and dear to my heart as I see consumers struggling everyday with the sometimes debilitating effects of lymphedema at MD Anderson Cancer Center where I work as Director of Rehabilitation Services. As AOTA explains, “Lymphedema is a complex, chronic condition affecting three to five millions of Americans. It results in the buildup and swelling of the affected body part due to the insufficient function of the lymphatic system. Untreated, lymphedema is progressive and can cause complications, comorbidities, and can impact an individual’s day-to-day functioning. It is most commonly caused by the removal of lymph nodes or vessels during treatment of cancer (AOTA, 2017, Online at: http://capwiz.com/aota/issues/alert/?alertid=73918626) Evidence shows that compression garments are highly effective in controlling lymphedema (Braveman & Hunter, 2017) but Medicare does not currently pay for compression garments. The Lymphedema Treatment Act would change this and provide critical coverage for patients with lymphedema. Take action now and urge your Member of Congress to support proper treatment of lymphedema! Visit: www.aota.org/take action today! Braveman, B. & Hunter, E. (2017). Occupational therapy practice guidelines for cancer rehabilitation with Adults. Bethesda, Maryland: AOTA Press.  Did you know that despite the critical role that occupational therapy plays in home health care and in helping consumers to stay in their homes safely, occupational therapy practitioners CANNOT open a home health case? According to AOTA, “Even when ordered on the plan of care, occupational therapists are not permitted conduct the required initial visit under Medicare. Additionally, they are not allowed to complete the comprehensive assessment unless OT is the qualifying service, such as under Medicaid or when OT is the qualifying service on a “continuing need” basis. Proposed legislation titled, “The Medicare Home Health Flexibility Act of 2017 (H.R. 3820/S. 977) change this and allow home health companies increased flexibility to use the most clinically appropriate skilled service to conduct the initial assessment visit and to complete the comprehensive assessment . Here is a link to an information sheet you can use to explain the problem: https://www.aota.org/~/media/Corporate/Files/Advocacy/Federal/Fact-Sheets/Medicare-Home-Health-Flexibility-Act-One-Pager-2017.pdf Go to www.aota.org/takeaction and contact your Senators and Representative and ask them to co-sponsor or support the Home Health Flexibility Act! Join me and take action!  Have you ever heard of the “pay go” rule? I hadn’t either until I logged into the AOTA Legislative Action Center at www.aota.org/takeaction. The “pay go” rule requires that any decrease in revenue such as tax cuts either must be paid for in other ways or automatic cuts happen in critical programs such Medicare, student loans and “safety net” programs. Right now both the House and the Senate have passed tax reform bills and leadership in both halls of Congress have indicated that this rule will not be enacted, but we can’t be sure and this is important! According to AOTA, “there are many issues competing for Congressional attention over the next several weeks: completion of tax reform, funding the federal government, raising federal spending caps, reauthorizing the Children’s Health Insurance Program, fixing Medicare policies such as the therapy cap, and working towards an agreement for the Deferred Action for Childhood Arrivals (DACA)” (Retrieved Online at: http://capwiz.com/aota/issues/alert/?alertid=79317626&PROCESS=Take+Action). We need to be sure that our Senators and Representatives hear from us and we need to let them know that waving “pay-go” is a must. This means they must take action and so must we. Go to the Legislative Action Center and you will find prepared text for an Email to send to your Senators and Representative. You can edit the text of the Email if you like but it is fast and easy. Stand up for our stakeholders and let your voice be heard!  We’ve dealt with the Medicare Therapy cap for the past 20 years and this is the year for us to put a stop to it! The arbitrary cap places an arbitrary limit of $1960 on the amount of outpatient occupational therapy a Medicare can receive each year, regardless of medical necessity or therapeutic need. Despite having an “exceptions process” in place, the cap creates extra costs and potentially harms clients who would benefit from occupational therapy services. We currently have bipartisan support in the “Medicare Access to Rehabilitation Services Act of 2017 (H.R. 807/S. 253)” which would permanently repeal the therapy cap. Sponsors and co-sponsors include Representatives Erik Paulsen (R-MN), Ron Kind (D-WI), Marsha Blackburn, (R-TN), and Doris Matsui (D-CA), and Senators Ben Cardin (D-MD), Dean Heller (R-NV), and Susan Collins (R-ME). According to AOTA, “In April 2015, Congress passed the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), which fixed other flawed Medicare policies, but failed to pass a permanent fix to the therapy cap. Despite strong bipartisan support for a permanent solution, Congress ultimately approved a two-tiered "exceptions process" through December 31, 2017” (AOTA, 2017: Online at http://capwiz.com/aota/issues/alert/?alertid=74944626). You can find talking points on repeal of the therapy caps at this link: https://www.aota.org/~/media/Corporate/Files/Advocacy/Federal/Tips-and-Tools/Therapy-Cap-Talking-Points-8-2-17.pdf Visit the AOTA Legislative Action Center at www.aota.org/takeaction to find contact information for your Representatives and Senators and Email them today! You can find editable text following this link: http://capwiz.com/aota/issues/alert/?alertid=74944626. By entering your home address, Email and phone number you can send an Email in less than 5 minutes! Join me by speaking out and asking to end the therapy caps now! I contacted my Congresspersons, now its your turn!  Today’s blog is about a critical role for the next Vice-President of AOTA; in fact it is a critical role for every occupational therapy practitioner and student.
BEING AN OCCUPATIONAL THERAPY ADVOCATE! For 33 years I have been an active advocate for occupational therapy, occupational therapy practitioners and our consumers. Each year, I participate in AOTA’s Capitol Hill Day. I have made 20 visits to Capitol Hill on Hill Day, in conjunction with AOTA Board of Director meetings and on personal visits to Washington D.C. This September I had the honor of acting as a mentor for two students who were making their first visit to the Hill. It was a wonderful experience. I am a longtime supporter of the American Occupational Therapy Political Action Committee (AOTPAC) and participate in the “two dollar a day” program. Last year I donated over $1,000 to AOTPAC. As Vice-President, I will continue to be highly engaged in advocacy. I will be highly engaged with AOTA members and non-members on social media, at State Association Conferences, at the AOTA Annual Conference & Exhibition and at other professional meetings such as the American Congress of Rehabilitation Medicine (ACRM) to encourage others to be active advocates. Please take a moment to visit www.aota.org/takeaction and spend a few minutes at the AOTA Legislative Action Center. Key issues currently being debated in Congress include the following (click the link to learn more):
Help me and other occupational therapy advocates to be more powerful professionals and take action now! Recently a photo of a past AOTA Board of Directors (the Board) was reposted on social media. The picture was taken at the AOTA Vision 2025 Summit in 2015. The photo includes all elected members of the Board at that time and two appointed members. Because the photo was “shared” a second time, it was not immediately evident that the picture was of the Board or where, when, and why it was taken. The photo received several comments including two that asked (I'm paraphrasing) “Where is the diversity?” One of the comments pointed out that there was no one included in the photo who had an obvious disability. Looking at the photo (which I am in) it seems apparent that the members of the Board at that time all or mostly outwardly appeared Caucasian. There seemed to be a range of ages and four of the 14 persons in the photo appear to be male. I think it is accurate to say that there is no one in the photo who appears to have an obvious disability (although we know of course that many disabling conditions are not outwardly visible). I was a participant in both the Centennial Vision retreats and the 2025 Summit. For this reason these comments immediately drew my thought to where we stand with diversity as a profession. It is a complex issue that I cannot fully address in one Blog post. I am sure that I will leave out some important information to consider in the big picture, but I want to share my perspective as a Candidate for AOTA Vice-President. This is meant as continuing the conversation, not wrapping everything up with a neat bow. First a few comments about the concept of diversity in the Centennial Vision driven from my personal experience. From my experience I remember that while the idea of becoming a diverse workforce most certainly included increasing racial, ethnic and gender diversity the concept was much broader. The concept of diversity in the Centennial Vision was meant to include all types of diversity including issues such as broadening the types of work settings in which occupational therapy practitioners work and/or recognizing the diversity that second career professionals bring to the workforce. It included diversity in terms of disability status. There were also mentions of recognizing other forms of diversity that are not immediately outwardly identifiable and becoming a profession that is fully welcoming of types of diversity such as sexual orientation or gender identification. This explanation is not intended to lessen the importance or the challenge of increasing racial, ethnic and/or gender diversity, it is simply an explanation of the origin of the concept of diversity in the Centennial Vision based on my participation in the Centennial Vision retreats and on the Board. I also want to state that the participants at both the Centennial Vision retreats and the Vision 2025 Summit (both groups near 100) were in fact diverse in many ways. So how have we done in becoming a more diverse workforce? We have made some identifiable strides forward, but clearly not the type of changes we saw in other areas of the Centennial Vision such as “widely-recognized” or “evidence-based.” In terms of diversity of practice settings we maintain strong footing in established areas of practice such as hospitals, schools and long-term care and in fact the percent of the OT workforce in hospitals and LTC/SNFS increased from 37.5% in 2010 to 46% in 2015. This graph is taken from the 2015 AOTA Salary and Workforce Survey (Online at https://www.aota.org/~/media/Corporate/Files/Secure/Educations-Careers/Salary-Survey/2015-AOTA-Workforce-Salary-Survey-LOW-RES.pdf). 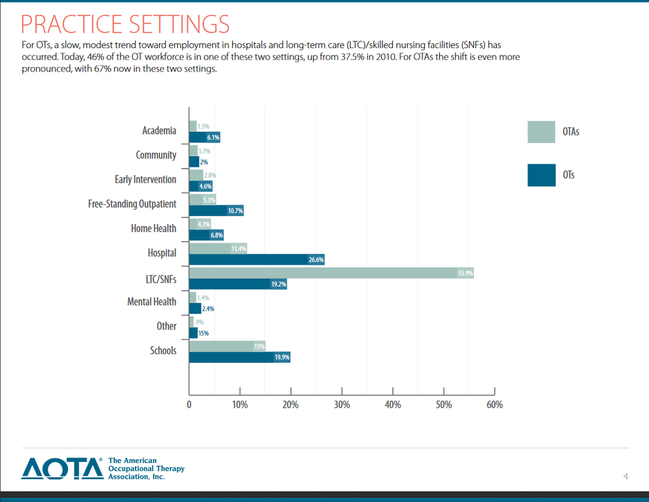 We have made forays into emerging areas such as primary care, population health and notably focused areas of practice such as oncology rehabilitation where I work. We certainly see many examples of creative practice with population such as refugees or the homeless. I continue to worry that we do not adequately support occupational therapy entrepreneurs and that private practice and business ownership receives less attention than it could. I am sure that many other examples of positives and areas for improvement could be mentioned. What about diversity in our students and new practitioners? I retrieved data through a search of AOTA Website on 12/6/17 and found a PowerPoint presentation with load date of 6/7/17 for a presentation given by Heather Stagliano (Director of Accreditation) and Neil Harvison (Chief Officer, Academic and Scientific Affairs) at the 2017 Annual Conference & Exposition in Philadelphia March 30-April 2, 2017. From 2000 to 2016 the number of occupational therapist students (including OTD) increased from 17,296 in 2000 to 20,627 in 2016 and the number of occupational therapy assistant students increased from 6,459 to 10,160 over the same time period. This next slide presents self-identified race according to the 2016 Annual Data Report from ACOTE. We can see that the percentage of students reported as white is approximately 75% overall. This is compared to 61.3% of people identified by the U.S. Census bureau in a population estimate for 2016 as “White alone, not Hispanic or Latino” (Retrieved Online 12/6/17 at: https://www.census.gov/quickfacts/fact/table/US/PST045216). 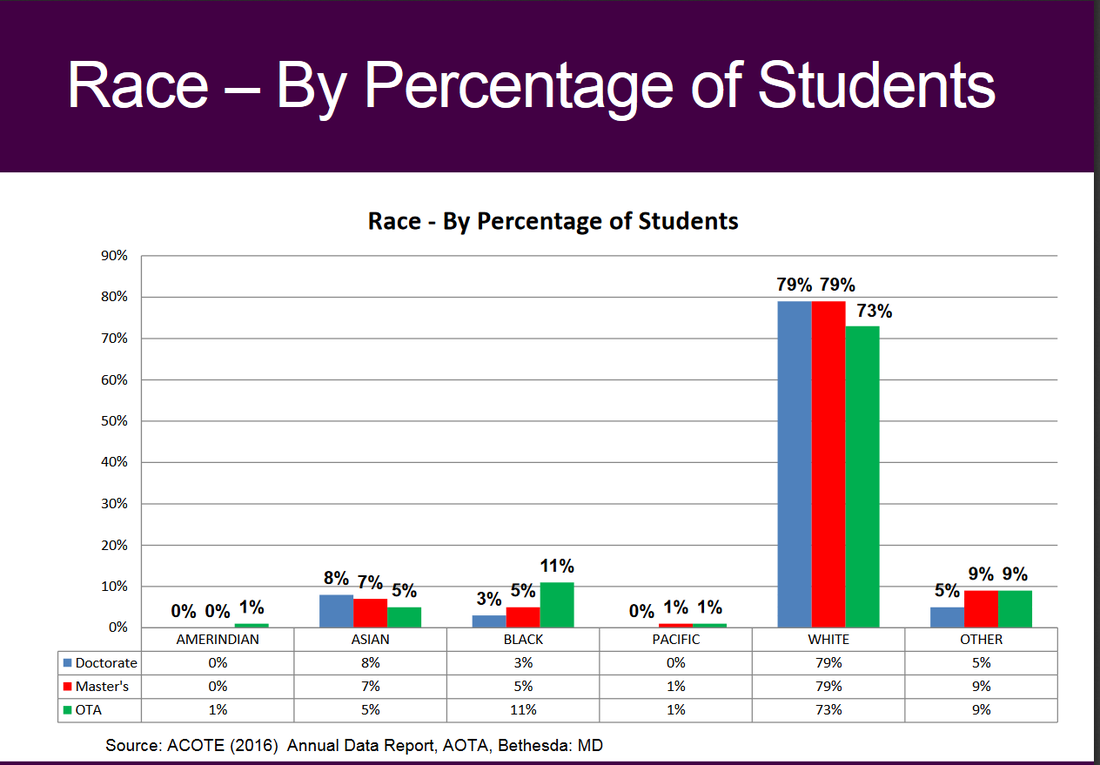 The next three slides show comparisons in percentages from 2010 to 2016 in those self-identifying as Hispanic, White, and Male. The next slide shows that the percentage of students self-identifying as Hispanic increased from 2010 to 2016. 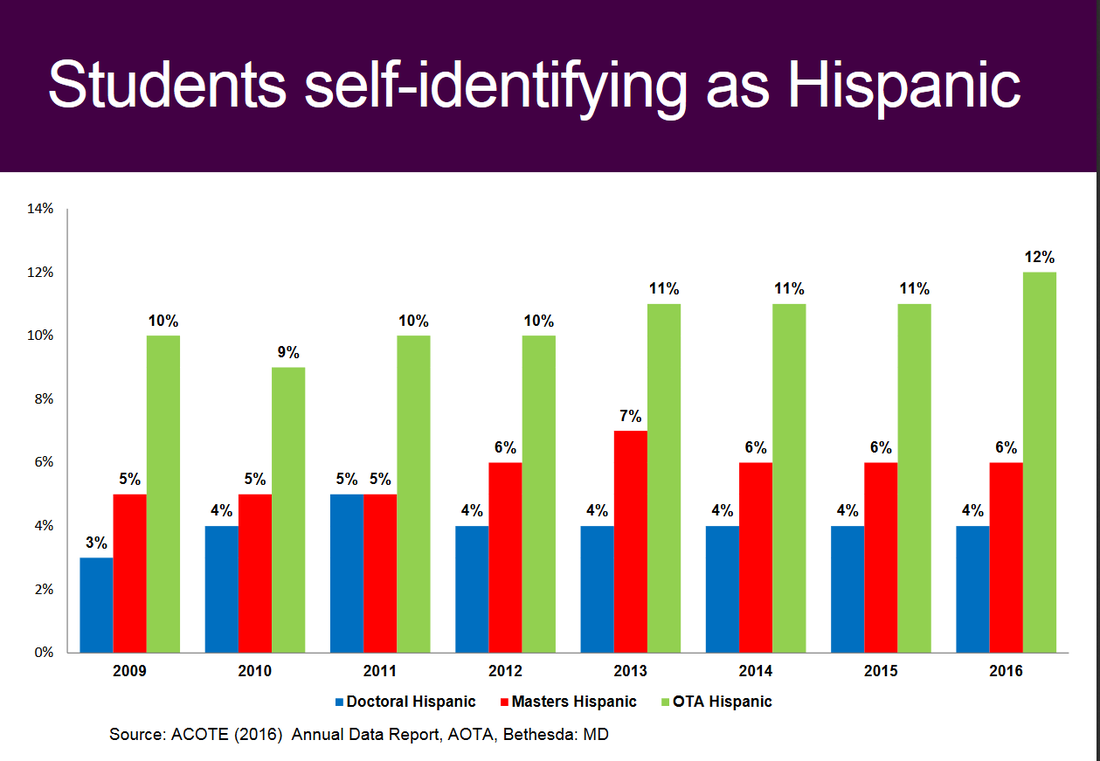 The next slide shows that the percentage of students self-identifying as White dropped from 2010 to 2016. . It is possible that some of this change could be explained by any changes in the categories included for self-identification (note that 5% of OTD students, 9% of Master’s students, and 9% of OTA students are identified as “other” in the slide on race from this report). 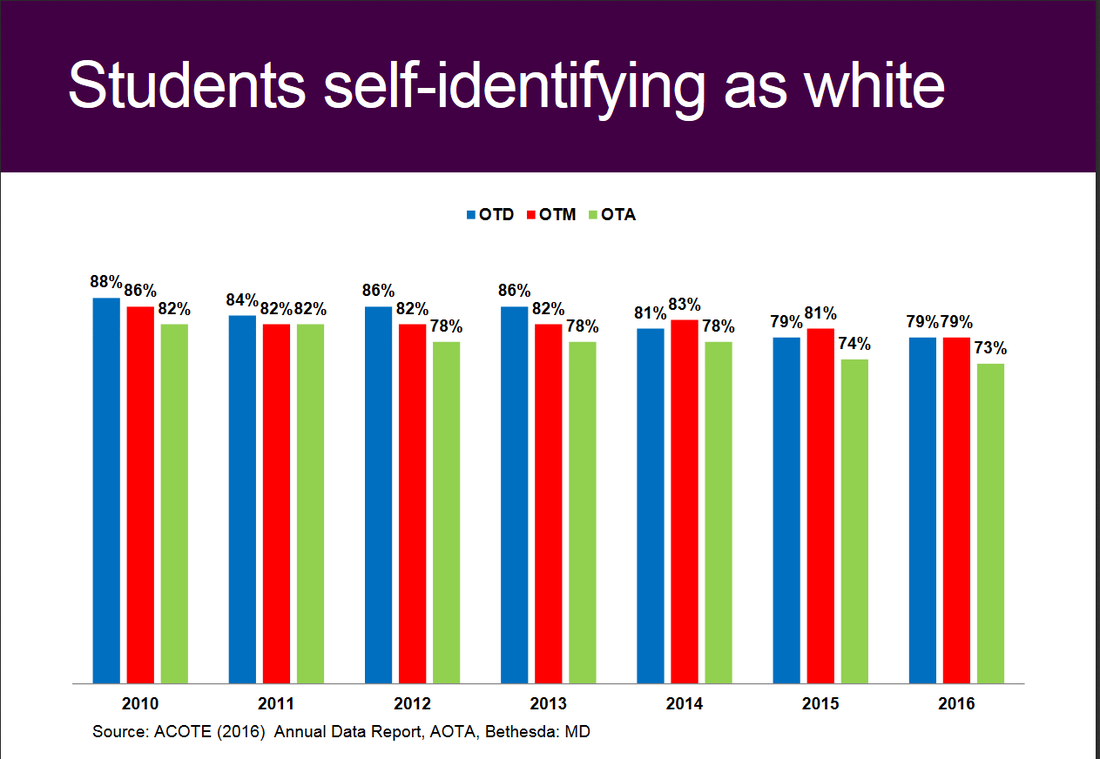 The next slide shows that the percentage of students self-identifying as male increased from 2010 to 2016 for OTD students, stayed the same for OTM students and dropped one percentage point for OTA students 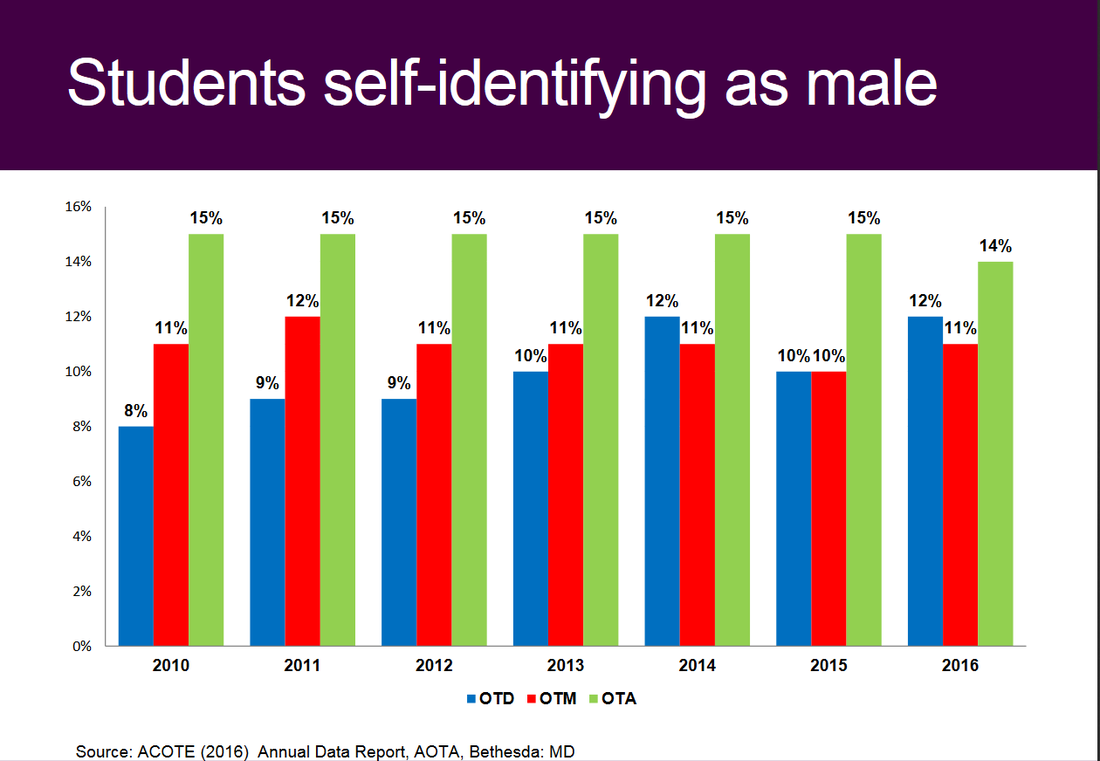 A full discussion of these statistics requires a deep dive far beyond the scope of this Blog post but I will summarize generally by saying that while we have made some improvements in these areas of diversity, I would characterize them as far from significant and leaving much room for improvement.
Before turning to some “so what” comments, I would like to comment on the issue of “obvious” or outwardly recognizable diversity and its complexity. Because I am included in the picture of the Board mentioned earlier and because I got to know my colleagues fairly well, I am positive that there are elements of diversity that are not outwardly apparent. These types of diversity are very important and should not be overlooked or undervalued. I want to avoid one of my pet peeves which is a “what about” response, meaning the tendency we have sometimes to respond to a concern about “A” with a response of “Yeah, but what about “B?” Still, diversity such as sexual orientation, gender identification, non-visible disability, ethnic diversity that may not be immediately outwardly recognizable ALL contribute in critical ways to making our workforce more diverse and more like the population in general. In this regard the answer to the question, “Where is diversity?” might be, “You’ll have to consider what you don’t see to see it.” So this Blog post has likely already run on too long, so let me get to the take-home, “so what?” messages that reflect some of my thinking as a candidate for AOTA Vice-President.
As a candidate for AOTA Vice-President I am committed to continuing attention and reinvestment of the efforts of the Board and the paid staff of AOTA in making our workforce more diverse. I would love to hear your ideas. Please contact me at [email protected], friend me or message me on Facebook or let me know if you would like to set a time to have an Online chat or phone call. Thank you. Before you vote for any candidate in the upcoming AOTA elections you should know their answer to two simple questions:
Why do I want to be the next AOTA Vice-President? First I have a sincere passion and deep belief in the distinct value that occupational therapy can offer our society. Second I believe that the most effective way I can contribute to our profession is through volunteer service to my professional association. I became hooked on occupational therapy as a junior in high school. After watching the movie “Brian’s Song” about a football player with cancer I decided I wanted to be a PT and began volunteering at the local community hospital. I was assigned to acute care outpatient and almost all of the treatment I saw involved basic ambulation of patients and A LOT of crutch training for sprained ankles and broken legs. I became disenchanted and decided to stop volunteering but the astute PT asked me why and convinced me to try volunteering in OT. All it took was two observation visits and I was set on what I wanted to do with my life. I marveled at the creativity, problem solving and the focus on what I know understand to be client-centered care. I didn’t know it then, but the OTs always involved their clients in occupation-based intervention and we performed ADLs, cooked meals, problem-solved grocery shopping, planned for being safe at home and for getting around my hometown of Bangor, Maine. I was the sort of kid who always wanted to lead. I was Student Council Vice-President and President of the Bangor YMCA Leaders’ Club. I was a very young Supervisor at the Bangor City Pools and volunteered for leadership participation in almost every endeavor. As is consistent with my character, I completed one of my three Level II fieldworks at AOTA in the Division of Continuing Education and got my first exposure to AOTA volunteer leadership and staff close-up. I benefited from amazing mentorship over the first few years of my career by my fieldwork supervisor Susan Robertson who had high expectations and confidence for what I could achieve! My first AOTA conference was 1986 as a practitioner with one year of experience. I listened to Katherine (Kitty) Reed give her Eleanor Clarke Slagle Lecture on the “Tools of practice: heritage or baggage?” and heard AOTA President Eleanor (Ellie) Gilfoyle address the audience on “Professional Directions: Management in Action” and discuss the value of creative partnerships. My first conference was an extraordinarily impactful event. My early experiences convinced me that occupational therapy has amazing potential to address society’s needs and that I could contribute to achieving that potential. An example was speaking to a large audience at the Kennedy Center in Washington, D.C. who had viewed the groundbreaking made for television movie about teen suicide “Silence of the Heart” and explaining the contribution of occupational therapy to preventing teen suicide. These beliefs were also why I chose to volunteer to be the Vice-President and then President of the District of Columbia Occupational Therapy Association (DCOTA) after just four years of practice. The association needed someone to volunteer and I stepped forward. My entire career has focused on developing occupational therapy programs and promoting the profession to achieve our potential. Today my passion is Vision 2025 and guiding the profession through our next steps towards meeting society’s occupational needs. I envision supporting practitioners in established areas of practice such as school systems, SNFS and hospitals while also promoting emerging roles in practice settings such as primary care and population health initiatives. We can do both, there is no need to choose and I have experience in both camps. All of my experiences have convinced me that my greatest potential for contributing to achievement of an aspirational future for occupational therapy is as a volunteer leader. After 33 years of practice and experience as a State Association President, Chairperson of an AOTA Special Interest Section, Chair of the Special Interest Section Council, Speaker of the Representative Assembly (RA) and AOTA Secretary I am ready to take my next step in achieving my potential as a volunteer leader as AOTA Vice-President. Why should you vote for me? So I am passionate and committed…but is that enough? Why should you vote for me for Vice-President? The answer mirrors the story of my passion and commitment. Campaigns are not the time for modesty, so I hope you will appreciate my confidence and taking this opportunity to promote my skills and experience. I have served as a direct care clinician in inpatient rehabilitation, acute care, inpatient psychiatry, a neonatal intensive care unit, a skilled nursing facility and two work rehabilitation programs. I have a broad understanding of occupational therapy intervention in a wide variety of settings. Today I work leading nearly 100 OT and PT practitioners and am connected to the daily real life challenges of today’s health care environment. I have been a manager in a community-based hospital, a large academic medical center, an entry-level educational program (as Program Director) and now as the Director of the largest and first ranked cancer rehabilitation hospital and research center. I am an expert in management and the management processes of strategic and operational planning, financial planning and management, personnel development, mentoring and management, continuous quality improvement, outcomes measurement and marketing and promotion of occupational therapy services. This is a critical skill set for the AOTA Vice-President who has traditionally been responsible for strategic planning, evaluation of the AOTA Executive Director and oversight of the Centennial Vision (now Vision 2025) activities. I have been an educator in a masters’ entry program and several post-professional clinical doctoral programs. I developed and delivered multiple courses. I guided the fourth ranked occupational therapy program through the accreditation process and have deep familiarity and working knowledge of the accreditation standards, the accreditation process and of the culture and climate of higher education. I was a researcher and developed multiple occupational therapy interventions that were tested through the implementation of $1.2 million dollars of federal research funding. I served on multiple NIH grant review panels and have represented AOTA and occupational therapy on expert panels for NIH and the National Cancer Institute. I have skills in academic leadership having served as a Program Director in one of the top rated educational programs in the country. I have a demonstrated history as a practitioner scholar developing and implementing funded research combining qualitative and quantitative approaches to demonstrate the distinct value of occupational therapy. Through these experiences I gained an understanding of the challenges faced by our occupational therapy scholars and scientists and what AOTA and AOTF can do to support them. I have been a consultant to multiple community-based organizations and educational programs. I served for 6 years on the Board of Directors of the Alexian Brothers’ AIDS Ministry and have guided Boards of Directors, state OT associations and multiple faculty groups through strategic planning and visioning. I was involved in the development of both the Centennial Vision and AOTA Vision 2025 as an elected AOTA leader. I have been a staunch advocate for occupational therapy on Capitol Hill, at State Houses, in federal agencies and in communities. I have been a front line advocate and mentored others in the process of advocating for the profession. I have visited Congress on behalf of AOTA and the profession for 20 years and have mentored others in advocacy. I have been a steady volunteer for state associations and for AOTA and have continually asked, “How can I help? What can I do to contribute?” I have pursued a path of progressive leadership consciously making decisions about the next challenge that I can take on to make a difference and to gain a new set of skills as a volunteer leader. I will bring this skill set to my daily work on your behalf. I served in the Representative Assembly as SISC Chair, as Speaker and as Secretary for a total of 11 years. As Secretary I served on the AOTA Bylaws, Policies and Procedures Committee (BPPC) as we went through a major Bylaws revision. I know our official documents inside and out and few AOTA leaders can match my working knowledge of these documents. I have a solid understanding of the philosophical base of our profession, our core values and the processes of developing and implementing theory-driven, occupation-based and evidence-based occupational therapy interventions. I was recognized in 2017 with the AOTA Recognition of Achievement Award for my contributions in program development. It is wonderful that we have a vibrant slate of candidates for Vice-President. What sets me apart and why you should vote for me is the combination of the experiences that I have had and the multiple advanced skills sets I have developed over 33 years. This is the right time for me to commit to being a servant leader and to give all I can to AOTA and our profession. I hope that I have convinced you of this as well, and that you will vote for me to be the next AOTA Vice-President! |
The opinions expressed in my blog are personal and neither represent the views of my employer nor any organization.
Archives
July 2023
Categories |

 RSS Feed
RSS Feed
Proudly powered by Weebly